


We can't protect our kids from everything, but we can and must protect them against COVID-19 injections
We can't protect our kids from everything, but we can and must protect them against COVID-19 injections

It is already more than one month ago that the Canadian Broadcasting Corporation (CBC) published an opinion piece titled “We can't protect our kids from everything, but we can and must protect them against COVID-19 infection”. In this op-ed, Dr. Alexander Wong, infectious disease physician in Regina, capital city of Saskatchewan, compares the risks of COVID in children to the risks of a preventable household accident. He blames himself for leaving his 3-year old son unattended for a moment near the kitchen stove, resulting in a severe burn. Although Dr. Wong admits that the risk of death from COVID is minimal for children, he advocates for the vaccination of 5-11 year olds that had just been approved in Canada — in order to “practically eliminate this risk”. I wonder what might be the benefit compared to the collateral damage when you attempt to reduce fatal outcomes from one specific virus from a statistical zero to another statistical zero?

My partner’s response to the article was the memory of how she was left unattended in the kitchen and pulled a step ladder to the stove to investigate what the grown-ups had told her not to touch. She’s been careful of burning herself ever since. The greatest harm I can see here is that the experience may have stifled her curiosity and ingenuity. No common-sensical parent would blame themselves, more than superficially, for such an accident. What parents should instead think about very carefully is who would be to blame if their children were to experience short- or long-term adverse effects from injections with an experimental, genetics-based COVID-19 designer drug?
Our group of Canadian Academics for Covid Ethics (CA4CE) has recently appealed to Ontario Premier Doug Ford to keep his “Hands off our children”. In another commentary, we explained “Five facts all parents should know about the mRNA vaccines”, including that the currently available products do not work like traditional childhood vaccines, do not provide immunity, and thus do not prevent transmission of SARS-CoV-2 (the basis of all vaccine mandates in schools, youth sports, and other “non-essential” environments); that their short-term safety has not been established and their long-term safety is unknown; and that following the precautionary principle with an oft-cited “abundance of caution” should prohibit any coercion towards injecting children at the present time.

Two days before publication of the cringeworthy CBC article, Toronto Sun opinion editor Anthony Furey called upon us to “Read what the kids' vaccine approval actually says”, noting that the recommendations by Canada’s National Advisory Committee on Immunization (NACI) were all but a “ringing endorsement” for the approval of the Pfizer/BioNTech product for the 5-11 years age group. NACI’s report indeed points out the very low risk of severe COVID and death in children. For example, this age group accounts for 7.5% of SARS-CoV-2 infections but only 0.007% of COVID-19 deaths in Canada, an under-representation by a factor of over 1,000. The report also notes risk factors for severe disease — “Down Syndrome, end-stage kidney disease, epilepsy, neurological disorders including motor neuron disease, multiple sclerosis, myasthenia gravis, and Huntington’s disease, as well as type 1 and 2 diabetes” and “Obesity (BMI >40)”. I am not sure of the prevalence of obesity among 5-11 year olds, but I am pretty certain that the other conditions are extremely rare and these families are already used to taking medical precautions in everyday life.
The NACI report then summarizes the Pfizer trial in school-aged children. This reads like a crime story and I leave it to each of you to make up your mind about this section (pages 5-8). For more information about Pfizer’s vaccine trials (not specific to the 5-11 years age group), I recommend the Canadian Covid Care Alliance’s (CCCA) documentation “More Harm Than Good” (video | slides). Most importantly, we need it be known that NACI’s recommendation to approve the injections was made despite their own conclusion from the clinical trial: “None of the identified cases met the pre-defined criteria for a severe case of COVID-19, therefore the data did not include estimates of vaccine efficacy against severe outcomes such as hospitalization, MIS-C or death.” In his opinion piece, Dr. Wong insinuates the opposite as he specifically mentions MIS-C from COVID-19 infection. But the fact is that we do not actually have valid proof that the vaccines prevent severe COVID or death in children aged 5-11.
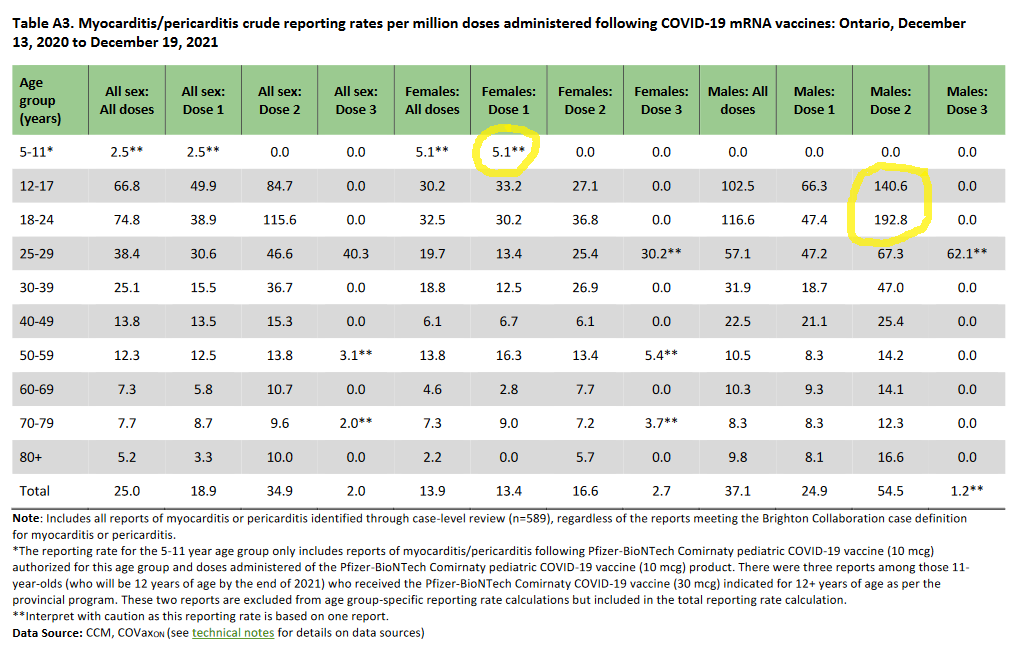
We do however know the damage caused by the injections. Dr. Wong mentions heart inflammation as the primary safety concern around the mRNA vaccines. He refers to Israel with an estimated 11 per 100,000 recipients aged 16-29. This is misleading at best, since we do not have to go overseas for better data. But maybe Dr. Wong and the CBC prefer that parents do not look too closely at Public Health Ontario’s weekly report on “Adverse Events Following Immunization”? The report with data updated to 19 December 2021 tells us that the myocarditis rate is currently as high as 193 per 100,000 males aged 18-24 from the second dose alone, or 240 per 100,000 for a two-dose course, which is 22 times the highest rate in the study from Israel. The next highest rate in Ontario is found in male teenagers aged 12-17 with 207 per 100,000 (19 times higher than Israel). Also note that the posted rates may represent a gross underestimation of the true rates, as argued e.g. by Koen Swinkels in “Public Health Ontario Is Not Being Honest about the Myocarditis Risk in Young Males” as early as October 1.
The vaccine dosage for <12 year olds was reduced (see the NACI report for the macabre history of that decision!) and their physiology may be different from the next-older group too. Indeed, the December 19 report, about 3-4 weeks into the stuttering kids’ vaccination campaign, contains no heart inflammation in 5-11 year old boys, yet one girl was affected as shown in the above table. Nevertheless, seeing all these issues in the vaccine safety and pharmacovigilance in Ontario/Canada, I would not knowingly subject my child to the expectable risk of harm from this intervention without any clear benefits.
Yesterday, one of the global leaders in cautioning against children’s vaccination for COVID-19, Dr. Robert W. Malone, was censored by Twitter. Dr. Malone is the inventor of the mRNA technology and thereby amply qualified to speak to its benefits and risks. One of his last tweets, which may have cost him the account, was a long list of references to peer-reviewed publications about adverse events in vaccinated children. Another tweet he wrote just before being suspended referenced the CCCA’s “More Harm Than Good” analysis of the Pfizer trials (see above). We need independent experts, critical journalists, and citizen scientists to monitor government and public health actions and their outcome. In completing the reading of the NACI report, it seems that there are some nuanced voices at the table, as the recommendations include an appeal to respect individual (family) decisions and treat people equitably. Unfortunately, this is one of very few positive elements in their report.
It is essential that children aged 5-11 years and their parents are supported and respected in their decisions regarding COVID-19 vaccinations for their children, whatever decisions they make, and are not stigmatised for accepting, or not accepting, the vaccination offer.
National Advisory Committee on Immunization, 19 November 2021, page 14