


Pfizerleaks: Natural immunity and the two-week "worry window"
Pfizerleaks: Natural immunity and the two-week "worry window"

Thanks to the “Naked Emperor” blog for making me aware of a document from the Pfizer/BioNTech “biologics licensing application” that was released by the US Food and Drug Administration (FDA) on March 24, somewhat out of line with the court-ordered monthly batch releases under a freedom of information request (see my previous Pfizerleaks post). The document is the REQUEST FOR PRIORITY REVIEW of the companies’ mRNA product, dated May 2021 in preparation for full FDA approval. The product, BNT162b2, is described as a “prophylactic vaccine” that targets the SARS-CoV2 virus, and the manufacturer claims that it generates “active immunization to prevent COVID-19 … in individuals >=16 years of age.”
In the subsequent text, the pharma corporations paint the picture of a severe, ongoing pandemic and make the case for a need to fully license the “safe and effective” vaccine, pointing to studies in mice and rats that showed disease prevention and no impact on reproduction. Among the details on safety, trials confirmed that the expected, short-lived, and “mostly mild to moderate” adverse events (AEs) were more frequent “and/or” more severe with increasing dose. I believe this is proof that the vaccine is indeed the likely cause of the observed AEs—something that pundits still dispute in the context of analyses of the Vaccine Adverse Events Reporting System (VAERS) data.
In the same Phase 1 safety section of the priority review request as well as with respect to the Phase 2/3 trials, and as noted by the Naked Emperor, Pfizer drops the comment that “Reactogenicity and AEs were generally milder and less frequent in participants in the older group (>55 years of age) compared with the younger group (≤55 years of age).“ I believe it was Dr. Peter Doshi who commented in a recent online webinar that in his view, the benefit-risk profile for young people is not acceptable based on the expected vaccine AEs alone, e.g. 1-2 days of feeling unwell, given this group’s extremely low risk from the disease, COVID-19.
The report also notes a “transient decrease in lymphocytes that was observed in all age and dose groups after Dose 1, which resolved within approximately 1 week”. Now if I believe Wikipedia, lymphocytes comprise core elements of our immune system, including T cells, B cells, and natural killer cells. Their temporary displacement or disappearance could obviously have detrimental rather than protective effects, e.g. if the vaccinee is exposed to SARS-CoV2 during the one-week time frame. In this context, the Emperor highlights that according to the FDA’s Emergency Use Authorization review memo, “SuspectedCOVID-19 cases that occurred within 7 days after any vaccination were 409 in the vaccine group vs. 287 in the placebo group.”
The Emperor rightly points to observed increases in case counts in many countries after the start of their vaccination campaigns. Independent health scientists, in particular Dr. Geert Vanden Bossche, have long warned that we should not conduct mass vaccination in the midst of a pandemic. The concern applies at an individual level, as suggested by the temporary drop in immune defenses after “immunization”, as well as the population level, where Vanden Bossche expects that the outdated vaccines could accelerate the development of escape variants of the virus.
The 7-day suppression of natural immunity suggested by the Pfizer trial data also reminded me of another blogger, the El Gato Malo. The bad cat most recently mentioned the “2-week worry window” in a February 13 post, after explaining it e.g. in “why ‘vaccinated covid deaths/hospitalizations’ are being counted incorrectly” on September 15, 2021. For example, a Danish study in long-term care home residents and health care workers found negative vaccine efficacy (i.e., increased risk of PCR test-confirmed SARS-CoV2 infection) within 14 days of the first dose of the Pfizer/BioNTech injection (see Table 2 of the preprint).
Now, speaking of natural immunity, the March 29 Naked Emperor post and Hill.TV April 4 Rising show’s host Kim Iversen made another observation of interest in the Pfizer priority review request. Among several sections reviewing vaccine efficacy, an updated analysis of the ongoing Phase 2/3 trial is included with respect to severe COVID-19 occurrences (at least seven days after dose 2). While the original trial data reported before the end of 2020 in conjunction with the American emergency use authorization did not have enough severe COVID-19 cases among participants to draw conclusions on vaccine efficacy, the updated data as per 13 March 2021 include 22 to 32 severe cases, depending on the definition. The key to the observation is that the counts among host without prior SARS-CoV-2 infection are the same as those “with or without” prior infection.
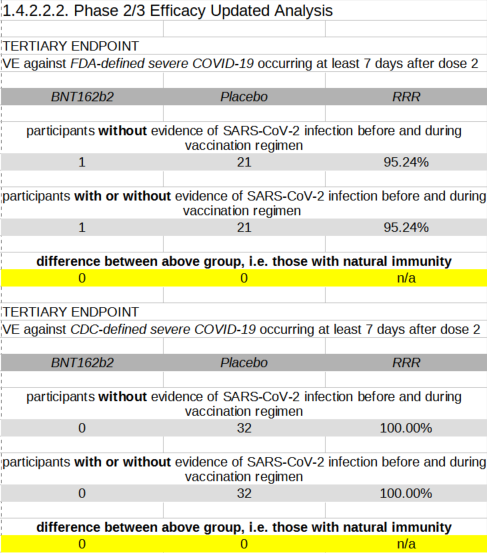
For the more stringent FDA-defined severe COVID-19, which according to Iversen is defined as patients requiring oxygen support, there was one case in the vaccinated trial group and 21 cases in the unvaccinated group, irrespective of whether participants with SARS-CoV-2 infection before or during the course of vaccination were included or not. In other words, of the participants who presumably acquired natural immunity through infection, none got a bad case of COVID-19 irrespective of the vaccine. Similarly, using the broader CDC definition based on hospitalization, there was no severe case in the vaccine arm of the trial and 32 in the placebo arm, yet this was also independent of whether those with prior infection were included. In other words, participants with natural immunity again were not found among the severe cases, including in the unvaccinated group.
In the preceding Section 1.4.2.2.1 of the same document, results from the original trial period regarding confirmed COVID-19, rather than severe COVID-19, were reported. These results do show a difference to the detriment of the placebo recipient, although the numbers are even smaller than those above. The trend from these two sets of trial outcomes suggests that natural immunity through prior infection does not prevent re-infection but protects against severe outcomes. This matches my understanding that immunity is not an on/off switch but a degree of protection, which depends on many external factors, such as circumstances of exposure, virus variant, general health, and early treatment. Coincidentally, the same indistinct outcome is what we get from the injections, which do not prevent infection nor reliably protect from disease, as shown in the cases and hospitalizations of vaccinated and boosted people during the current wave. Isn’t it about time to respect and celebrate natural immunity to SARS-CoV-2 in North America?