


Lockdowns, Distancing, and Face Masks - Better Sorry Than Safe?
Lockdowns, Distancing, and Face Masks - Better Sorry Than Safe?
With non-pharmaceutical interventions against SARS-CoV-2, we are pursuing futile precaution at the cost of focused protection.
In an interview for the documentary "Planet Lockdown", retired epidemiologist Dr. Knut Wittkowski mentions the subtitle of the famous play, "The Barber of Seville". The subtitle "The Futile Precaution" refers to the literary theme of an older man's useless attempts to prevent his young wife or love interest from running away with a younger man. The non-pharmaceutical interventions (NPIs) --- lockdowns, "social" distancing, and face-covering --- mandated to slow the spread of SARS-CoV-2 increasingly feel like such a futile attempt at stopping a respiratory virus from running its course. As Dr. Wittkowski notes, "we have seen that theme be played on the largest stage possible, the entire world!"
To cope with the "world ... gone bonkers" (quoted from Dr. Malcolm Kendrick), I signed up for daily emails from one-of-a-kind libertarian Tom Woods. His confident bashing of "lockdown supporters" has been quite uplifting among the dissonance of zealous-hysterical fear-mongering found across the (social) media. For months now, Woods has been promoting the work of twitterer Ian Miller. Miller shares graphs of daily new "COVID-19 cases" for different countries, US states and counties, and the occasional Canadian province, with markers for noteworthy policy changes such as the beginning and end of mask mandates; public news and statements about mask effectiveness; or major holidays or sports events that were expected to result in "spikes" of cases. The graphs unfailingly show no difference between the curves of states that pursued different approaches; no outbreaks after the lifting of lockdowns and mask mandates; but conversely epidemic curves increasing dramatically despite government restrictions. A small selection is shown here.
Famously, the governors of South Dakota and Florida were reluctant to implement lockdown measures and/or quick to lift them after the first wave of SARS-CoV-2. Comparing e.g. South Dakota with its neighbour North Dakota, or Florida with California, with respect to their population-adjusted COVID-19 cases or deaths, shows essentially the same curves. Infamously, in early March US President Biden accused the governors of Texas and Mississippi of "Neanderthal thinking" for their decisions to lift COVID-19 restrictions. He called on the states to "follow the science", which is what two of Ian Miller's charts' labels refer to. The result, of course, being that the "Neanderthal states" did as well as, or better than, the "science states". Taking it a notch beyond the static graphs, Tom Woods created the interactive COVID Charts Quiz, in which the viewer is asked to guess the pandemic response stringency or the timing of measures based on undated, unlabeled epidemic curves.
The United States are a large country with a significant amount of political power decentralized at the state level, which allows for informative comparisons. Owing to the geographic extent of the US, comparisons between neighbouring, or otherwise similar, states are feasible. In Do Lockdowns Make a Difference in a Pandemic?, Maria Krylova develops criteria for suitable comparisons between jurisdictions, including similar population size, geographical location (latitude) and climate, type and magnitude of the economy, degree of urbanization, and political orientation. In addition to California-Florida and Krylova's Minnesota-Wisconsin comparisons, Canada's Province of Quebec appears to be quite comparable to the country-of-interest Sweden based on these criteria. While no-lockdown Sweden has almost 2.5-times the "cases", it is within 10% of curfewed Quebec's death rate, with 144 deaths per 100,000 population compared to the Belle Province's 131 (data from Government of Canada and Worldometers as of 26 June 2021).
Incidentally, both Quebec and Sweden badly failed to protect vulnerable seniors living in longterm care homes. A report by the Canadian Institute for Health Information (CIHI) notes that Quebec leads among Canadian provinces with 9.5% of all seniors 65 years and older living in longterm care homes, and longterm care home deaths accounting for 70% of all 1st-wave COVID-19 deaths as of 25 May 2020. The latter percentage was the same for Ontario, and the province was faced with a scathing report from the Canadian military after they were called in to help manage all-but-abandoned facilities, followed by a comprehensive review of the decades-long neglect of the province's nursing homes. Another CIHI report for the 1st and 2nd waves of COVID-19 up to 15 February 2021 pegs the number of COVID-19 deaths in longterm care and retirement homes at 14,739 out of Canada's total of 23,110 fatalities (69%). This fact reflects the skewed age distribution of SARS-CoV-2 victims and clearly suggests focused protection of the well-defined vulnerable groups -- the elderly and those with pre-existing health conditions --, as argued by numerous critics of the blanket non-pharmaceutical interventions used in Canada and elsewhere.
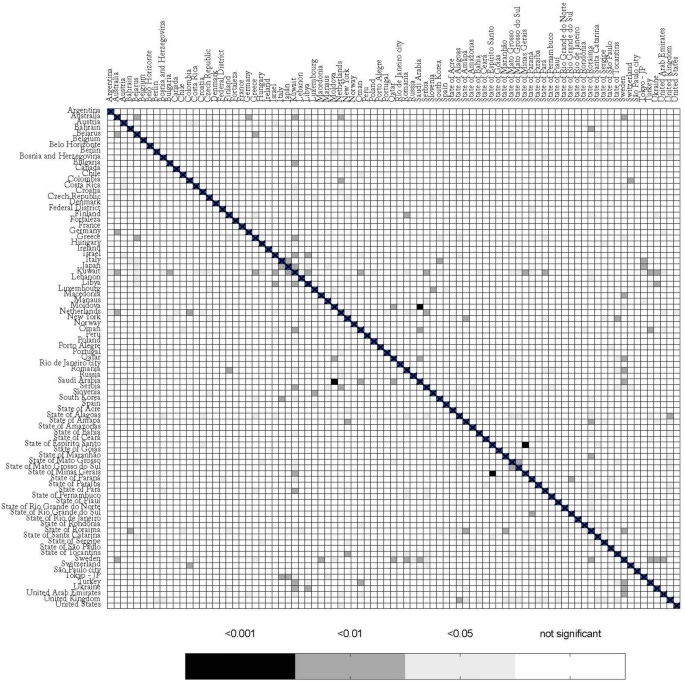
There is a lot of evidence that lockdowns, mask mandates, and social distancing did not slow or stop the spread of SARS-CoV-2. An annotated bibliography titled "Lockdowns Do Not Control the Coronavirus: The Evidence" was published in December 2020 by the American Institute for Economic Research. Their sources are based on a collection of publications initiated by longtime lockdown sceptic Ivor Cummins. For example, in a study published in Nature in March 2021, researchers found only minimal associations between mobility restrictions and COVID-19 deaths when assessing 3741 pairwise comparisons between 87 regions around the globe and therefore titled their article "Stay-at-home policy is a case of exception fallacy".
Furthermore, evidence is beginning to appear that the non-pharmaceutical interventions along with specific response measures actually had a detrimental impact. In addition to anecdotal evidence collected e.g. at https://collateralglobal.org/, started as a sort of companion site to the Great Barrington Declaration, we'll have a look at two papers written in June and August 2020 by Dr. Denis Rancourt, titled "All-cause mortality during COVID-19: No plague and a likely signature of mass homicide by government response" and (with co-authors) "Evaluation of the virulence of SARS-CoV-2 in France, from all-cause mortality 1946-2020".
Assessing all-cause mortality data from the US, France, and other European countries, the authors argue that longterm mortality patterns suggest that the first COVID-19 deaths peak in March 2020 cannot be explained by the natural cycle of respiratory diseases. They suggest that the abruptness of the peak and the fact that it occurred at greatly different magnitudes in different jurisdictions must be due to pandemic response policies and procedures. Rancourt et al. argue that quarantine and isolation procedures in institutional settings killed vulnerable elderly residents through stress and lack of social interaction. Many months later, a CDC report on underlying medical conditions of COVID hospitalizations (link goes directly to Table 2) finds that "anxiety and fear-related disorders" were the second highest risk factor for deaths, after obesity and ahead of diabetes. Fear and stress are wellknown risk factors for human wellbeing; on this basis alone, much of the public health messaging that was, and continuous to be, amplified by the media to pressure the population into compliance with social and mobility restrictions and mass vaccination is fundamentally misguided. In addition, it is becoming increasingly clear that the ad-hoc measures taken to "protect" longterm care homes and similar facilities had a deadly impact on their residents.

Canada too has markedly different COVID impact between its provinces, even after adjusting for population. Quebec's rate is some 50% greater than Manitoba's, which is some 20% above the national average, followed by Ontario, Alberta, Sasketchewan, and British Columbia with the lowest rate at only one-quarter that of Quebec. The stringency of mobility restrictions is somewhat inversely related to these COVID death rates; causality, if it exists, could point either way: deaths caused by lockdowns, as discussed above, or conversely, restrictions being tightened as a consequence of deaths rising due to other causes. Nevertheless, the great differences in death rates support Rancourt et al.'s argument that different medical procedures and non-medical measures as well as systemic differences had a great impact on COVID mortality.
Still in Canada, our venerable statistics agency in The Daily released 10 March 2021 actually found that from September to November 2020, there were excess deaths beyond the COVID deaths count, thus not explained by direct impact of the virus. Based on the preliminary numbers, the unexplained deaths among a total of 3,625 excess deaths could be close to 1,800 in those three months, although updated COVID statistics suggest this number could be closer to 600. This lower number is based on my review of Our World In Data, which now reports around 3,000 COVID deaths for Sep-Nov, instead of Statistics Canada's 1,835 deaths at the time the report was issued. In conjunction with a shift to a younger demographic (men < 45 yrs, women 45-60 yrs) among the excess deaths, Statistics Canada speculates about the "indirect consequences of the pandemic" and refers to reports about rising drug overdose deaths in several provinces. I trust you will agree that these observations contribute another concerning element to our assessment of lockdowns.

It has been noted that the cost-benefit or risk-benefit calculation of NPIs is nowhere near clear-cut. I am not aware that such an analysis was officially conducted by any government worldwide. For example, Ottawa Public Health recently admitted that they have no record of such a calculation for the decision on a mask mandate in public places. However, several independent researchers have published formal cost-benefit analyses of lockdowns. The negative impact ("cost") of lockdowns is measured in years-of-life lost over periods of decades, rather than the shortterm excess mortality reported above. In "COVID-19: Rethinking the Lockdown Groupthink", Dr. Ari Joffe, pediatrician at the University of Alberta in Edmonton, estimates 5-10 times more "wellbeing years" lost than saved. In "Covid Lockdown Cost/Benefits: A Critical Assessment of the Literature", Dr. David Allen, economist at Simon Fraser University in Vancouver, pegs the costs at up to 282 times the benefit.
Both the cost and benefit sides of these equations are greatly uncertain. As an example, there is no consensus on the burden of COVID itself. Germany's corona deaths were on average 83 years old. The infectious disease agency RKI calculated the years of life lost using an average of 9.6 years of remaining life expectancy for each COVID death -- a highly questionable assumption. By contrast, mathematician Dr. Günter Eder estimates a remaining life expectancy of only 10 weeks (!) for the 85% of COVID deaths who had significant comorbidities and applies the 9.6 years only to those 15% who were healthy when hit with COVID. Eder's 66,318 years of life lost contrast sharply with the RKI's 303,608 YLL. What's more, 2,724 people died in traffic accidents in Germany in 2020 despite mobility restrictions. Their average age was 51 and assuming a representative sample of the population, they would have had a remaining life expectancy of 30 years, resulting in a toll of 81,720 YLL. Thus, according to Eder's estimate, traffic cost more life years than COVID in Germany in 2020, despite all mobility restrictions!
The flap of a butterfly wing in one location can create a storm in a far-away location. "Understanding the Butterfly Effect" in chaos theory involves two distinct aspects that can both be linked to the corona crisis. Meteorologist Edward Lorenz used it to illustrate the large possible impact of small changes in measurements and/or model inputs. During the COVID pandemic, we keep seeing epidemiological models badly fail in predicting case counts. The butterfly effect also exemplifies the connectedness of complex dynamic systems. Human communities and the human body are highly complex socio-economic and biological systems, respectively. Interfering with such complex systems by enforcing untested NPIs or pushing experimental vaccines is a high-risk gamble.
As an inane example, according to Best Health magazine (see figure) , our bodily microbiome may have changed due to the reduced variety of microbes we are exposed to with social distancing rules in place. Other side effects of the pandemic response are more serious. I am worried that it's hubris that we attempt to stop the course of a respiratory disease. Rather than deploying the blunt and destructive arsenal of non-pharmaceutical interventions, we should have stuck to our guns: basic hygiene procedures; staying at home when sick; standard targetted protections for the elderly, vulnerable persons, and health-care workers; development/deployment and continuous revision of available medications and treatment plans. COVID-19 would have quickly lost its terror.