


COVID-19 — Who's in Charge?
COVID-19 — Who's in Charge?
A Checkup on the Qualifications of Ontario's Medical Officers of Health

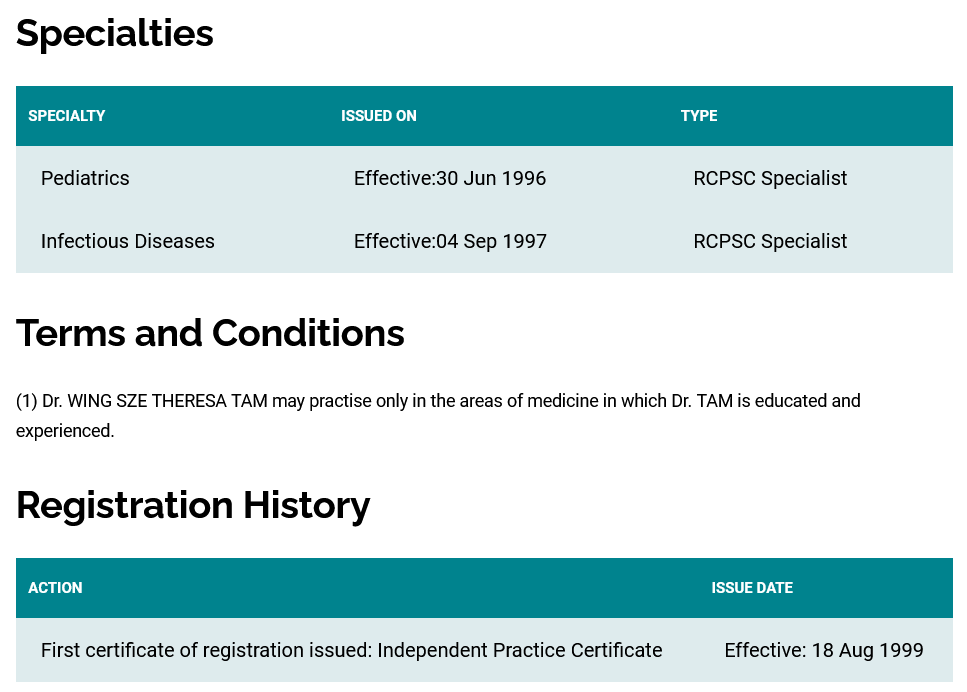
In a June 14 interview with independent journalist Eva K. Bartlett, Dr. Denis Rancourt explains that physicians in Canada are only allowed to practice in the area of medicine, in which they are formally trained and certified. In that interview and a June 23 series of tweets, he points out that Dr. Theresa Tam, Chief Public Health Officer of Canada, appears to be practising medicine illegally. Her specialties recorded in the College of Physicians and Surgeons of Ontario’s (CPSO) database are pediatrics and infectious diseases, and the College clearly states that Dr. Tam “may practice only in the areas of medicine in which [she] is educated and experienced”. Meanwhile, the field of public health, in which she is arguably practising, is the subject of a distinct specialization in “Public Health and Preventive Medicine“, or its older version, “Community Medicine”.
According to a Canadian Medical Association pamphlet, “Public health and Preventive Medicine (PhPm) is the branch of medicine concerned with the health of populations”. The specialization requires completion of a five-year residency program accredited by the Royal College of Physicians and Surgeons of Canada. Importantly, the “patient” of a public-health physician is not an individual but the population. The field is inherently holistic; it integrates “skills in leadership; development of public policy; design, implementation and evaluation of health programs and applies them to a broad range of community health issues”. This is quite different from the expectations of a pediatrician or infectious disease specialist such as Dr. Tam, and the CPSO explicitly requires both, education and experience in the specialty, thus e.g. on-the-job experience in public health administration alone would not be sufficient for someone to qualify for the top job.
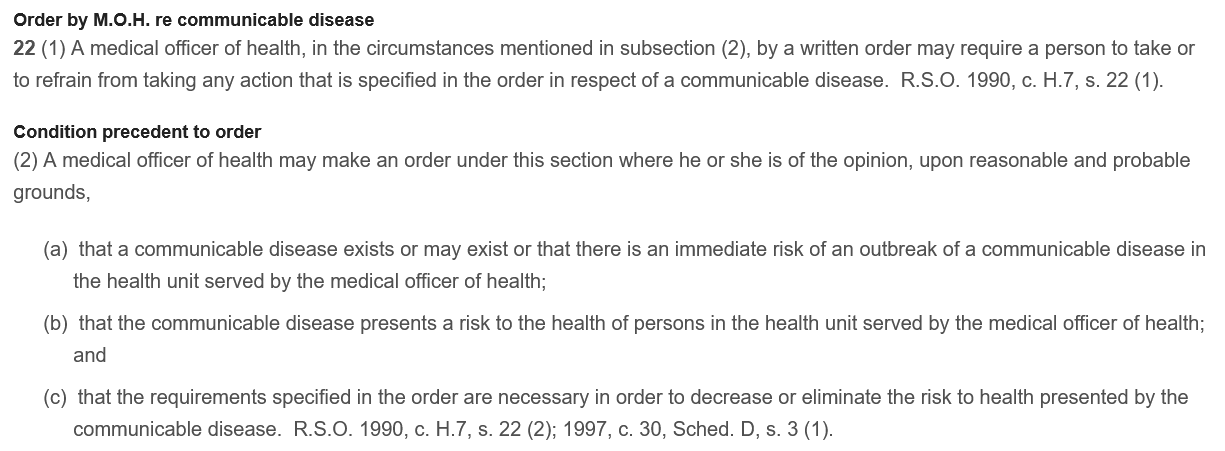
In the province of Ontario, there are 34 public health units, each directed by a medical officer of health (MOH) who has extensive powers granted by the Health Protection and Promotion Act. Without deeper insight into other applicable laws and regulations, I note that Section 22 HPA allows each MOH to tell anyone within their unit what they must, or must not, do “in respect of a communicable disease”. This applies if the MOH reasonably believes that there “exists or may exist” (emphasis added) a communicable disease that presents “a risk to the health of persons”. There is no qualifier for the health risk, e.g. “serious”, nor for the number of persons affected, e.g. “a large number”. In essence, our trusted MOHs are invited to wield their powers whenever they please.
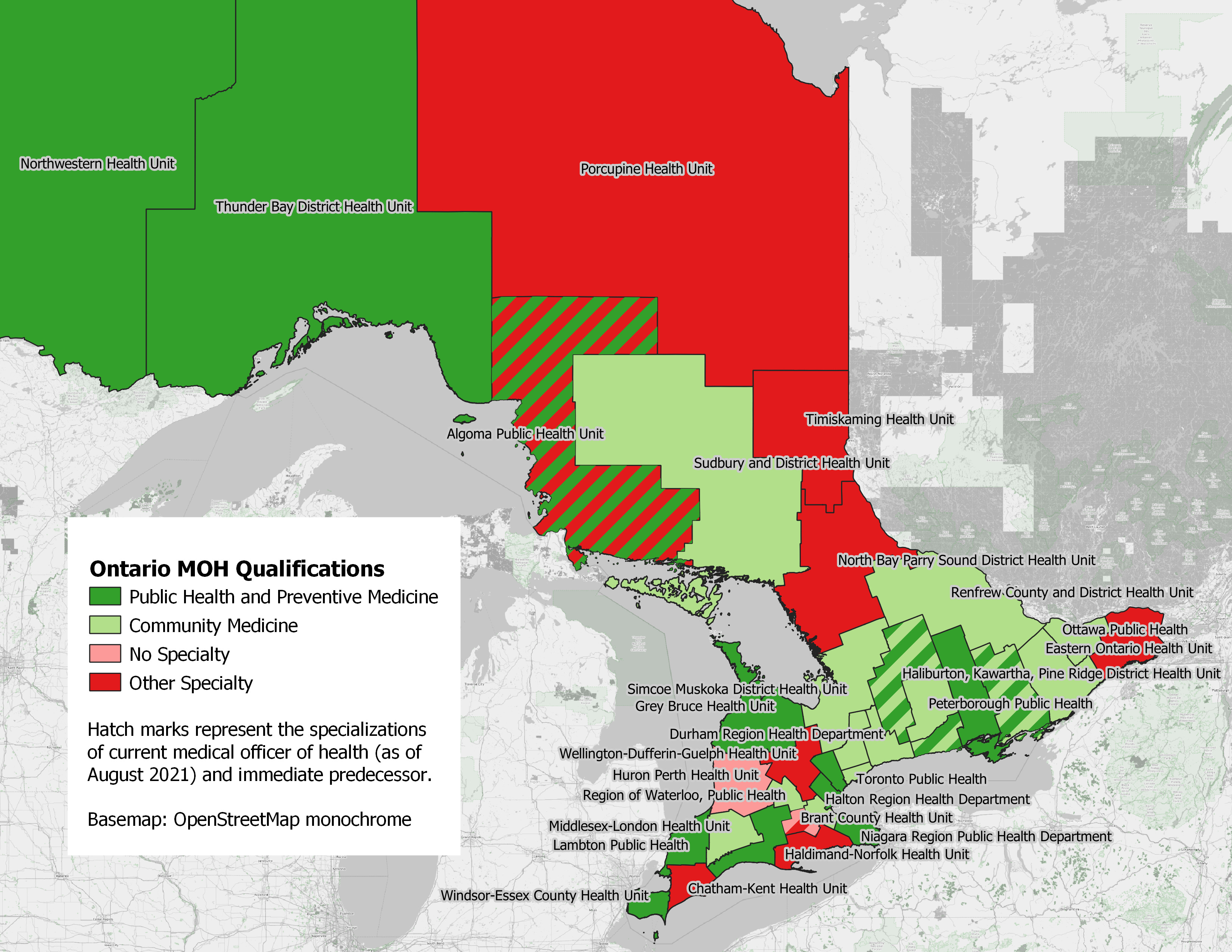
In this light, I was curious regarding the qualifications of these men and women. I started this analysis quite a while ago and had to look everyone up again later, as there seems to be significant turn-over in the MOH positions. The map above and data table below represent the information as of August 2021 and are provided for general information only. At that time, 7 out of 34 MOHs did not have PhPm or community medicine as their specialty (red areas on my map). Their training ranged from medical microbiology and anesthesiology to family medicine and pediatrics. Another two MOHs had no specialty according to the CPSO (pink areas). In addition, three former MOHs, also in office during a significant part of the COVID-19 pandemic, had ineligible specialties: physical medicine/rehab and family medicine.

The province’s Chief Medical Officer of Health, Dr. Kieran Moore, is shown in the table as the previous MOH for Kingston, Frontenac, and Lennox and Addington Health Unit, where he served before he was appointed to the provincial top job in May 2021. He holds the community medicine qualification. This should enable him to maintain an evidence-based, comprehensive perspective on all aspects of public health as I have personally experienced it working with staff at the “healthy public policy” directorate at Toronto Public Health. Indeed, in a memo dated Aug 31 but publicized only two months later, Dr. Moore accepts the similar degree of infectiousness in unvaccinated and fully vaccinated “breakthrough” cases (perhaps better characterized as “vaccine failure” cases!). More recently, in a Oct 28 press conference, Moore also acknowledged the effectiveness and value of natural immunity, as discussed e.g. in this Rebel News article.

In addition to the legal question, whether some of our medical officers are practising medicine illegally, this post also questions the preparations of these public health doctors in leading society through the ongoing crisis. It comes down to a question of expertise: What expertise(s) is/are needed for different analysis, planning, and decision-making tasks? As I have noted before, with reference to retired Alberta emergency manager Dave Redman, we are in a public crisis, not a public health crisis. This makes it necessary to consult with experts across numerous disciplines. It explains why e.g. geographers, aerospace engineers, theologians, or economists are analyzing and opining about COVID-19. Within the health aspects of the crisis, health and affiliated natural scientists provide input that remains largely unheard, as do concerns from practising MDs and nurses.
The field of public health should ensure strategic, holistic direction beyond the views of a narrow medical field. Unfortunately, with or without the proper qualifications, our MOHs appear to be irrationally focused on one virus, one disease, and one solution. Not surprisingly, given the destructive pandemic response, calls for the resignation of MOHs are rampant, including my colleagues’ open letter to public health officers (“What have you done?!”) and Irvin Studin’s “Ontario's medical officers of health must resign”. Many have written about the longterm damage inflicted on people’s trust in public health, with Jeffrey Tucker’s “The Collapse of Trust in Public Health” for the American Institute of Economic Research being one of the more pointed essays.