


The long shadow of the "common good"
The long shadow of the "common good"
On the principles of medical ethics, red lines in an ethical pandemic response, and the difficulty of having a healthy debate about responsible public health

In a recent Zoom meeting with a small group of critical public health scholars and practitioners, the topic of medical ethics came up — again. As everyone is looking at the COVID-19 pandemic through their own expertise and/or experiences, those holding on to the canonical principles of medical ethics have had a rough ride due to the many transgressions committed in the last three years.

As a relative novice, I found an outline by Santa Monica ophthalmologist and biomedical research scientist Dr. Houman Hemmati to be quite helpful. The basic principles of medical ethics, according to Dr. Hemmati’s Twitter thread, are as follows (lightly edited with bold/italic emphasis added, while all-caps are from the original):
You cannot administer or even recommend a medical treatment, including a vaccine, without full informed consent from adults, or parents, and assent in the case of children who can understand.
Informed consent requires a thorough understanding of the risks, benefits, and alternatives to that medical treatment. Alternatives could include NO treatment. [This information] must be given in a manner that the patient can fully comprehend.
Informed consent cannot happen when there is any direct or indirect coercion. Indirect coercion would include threatening someone's job, or ability to travel, or paying someone a meaningful amount of money. To someone poor, even $20 could be considered coercive.
Patient autonomy must be respected. If someone FULLY understands risks/benefits/alternatives to a treatment yet decides not to take it, that person CANNOT be shamed/punished/coerced/extorted.
If a doctor or public health official/agency doesn’t fully believe that the known/likely benefits of a treatment to that specific patient outweigh the potential risks, they shouldn’t recommend that treatment or even refuse to administer if zero/minimal benefit with risks.
It is morally criminal to administer any medical treatment (with exception for imminent life/death or few others) to a child without assent (if possible) and parental informed consent. [Health care providers] cannot shame, coerce, bribe or trick or ask not to tell parents.
Dr. Hemmati then observes quite accurately:
When COVID hit, much of society suddenly thought it’s perfectly ok to fully suspend medical ethics ‘for the greater good’ or ‘out of an abundance of caution.’ Zero regard for having any knowledge of [the] risks/benefits and zero individual autonomy. Our leaders also used this suspension of medical ethics to divide us into good (obedient/compliant) and evil (questioning, requesting informed consent, refusing treatments for themselves/kids). What happens to societies that do this? They collapse. People turn against one another.
Since Dr. Hemmati is American, let’s verify that his views on medical ethics during a pandemic apply to Canada too. Quite some time ago, a colleague had made me aware of the Public Health Agency of Canada’s (PHAC) “Public health ethics framework: A guide for use in response to the COVID-19 pandemic in Canada”. That page was updated in August 2022, but its first archived version dates back to June 2020.

The introduction of the guide recognizes the difficult situation that policy-makers, public health administrators, and health-care providers were facing near the beginning of the pandemic:
The public health threat posed by the COVID-19 pandemic has led all levels of government to take unprecedented measures to help slow the spread of COVID-19 and thereby minimise serious illness, death and social disruption resulting from the pandemic. Difficult choices are being made in a context of considerable uncertainty, as knowledge about COVID-19 and the impact of unprecedented public health measures evolves rapidly. Examples include decisions about allocation of scarce resources, prioritization guidelines for vaccines and medical countermeasures, curtailment of individual freedoms, and closing or re-opening public spaces, schools and businesses. Recognizing the fundamental ethical nature of these choices can help decision makers identify competing values and interests, weigh relevant considerations, identify options and make well-considered and justifiable decisions.
The guide then acknowledges two guiding values: trust and justice, as well as four ethical principles: respect for persons, communities and human rights; promoting well-being; minimising harm; and working together. These are followed by four criteria for “weighing options” to promote well-being and minimise harm: effectiveness, proportionality, reciprocity, and precaution. Lastly, five procedural considerations are proposed: accountability, openness and transparency, inclusiveness, responsiveness, and intersectionality.
Perhaps owing to my own expertise in decision support systems, I find the four decision-making criteria particularly important. Effectiveness is defined as the “reasonable likelihood that the proposed decision or action will achieve its goals, and that its implementation is feasible.” If you measure vaccine passports or workplace vaccination mandates against this criterion, decision-makers have failed us badly. Whether you assume the goal was to actually “stop the spread” or just to slow infections or generally keep everyone “safe”, it was known from the beginning of the vaccination campaign that the COVID-19 shots were non-sterilizing and had not been tested for efficacy against transmission.
Proportionality requires that “potential benefits should be balanced against risks of harm.” In addition, “Measures should be proportionate to the relevant threat and risks, and the benefits that can be gained.” Did general lockdowns and school closures meet this criterion? One of Dr. John Ioannidis and team’s latest papers points out that 94% of the world population is less than 70 years old. The researchers recalculate SARS-CoV-2 infection-fatality rates for this vast majority of the population and find that they were all but negligible. In other words, a proportionate response to COVID-19 back in 2020 would have focused on protecting the small, vulnerable segments of the population as advocated e.g. by the Great Barrington Declaration.
The reciprocity criterion speaks to societal support for those facing greater risks or burdens than others. This could be interpreted in different ways, one of which could have been to better support elderly and immunocompromised people while letting everyone else continue their normal lives, for the benefit of all.
Lastly, the precaution criterion is presented in a skewed fashion: “scientific uncertainty should not prevent decision makers from taking action to reduce risks associated with COVID-19.” Instead of supporting action for action’s sake, the ethics guide should have emphasized that the precautionary principle fully applies to the measures taken, including the early restrictions. It is now widely acknowledged that Sweden’s cautious (!) approach to lockdowns and school closures benefited the country in the long run with low excess mortality, as predicted by its chief public health officer from the beginning of the pandemic.
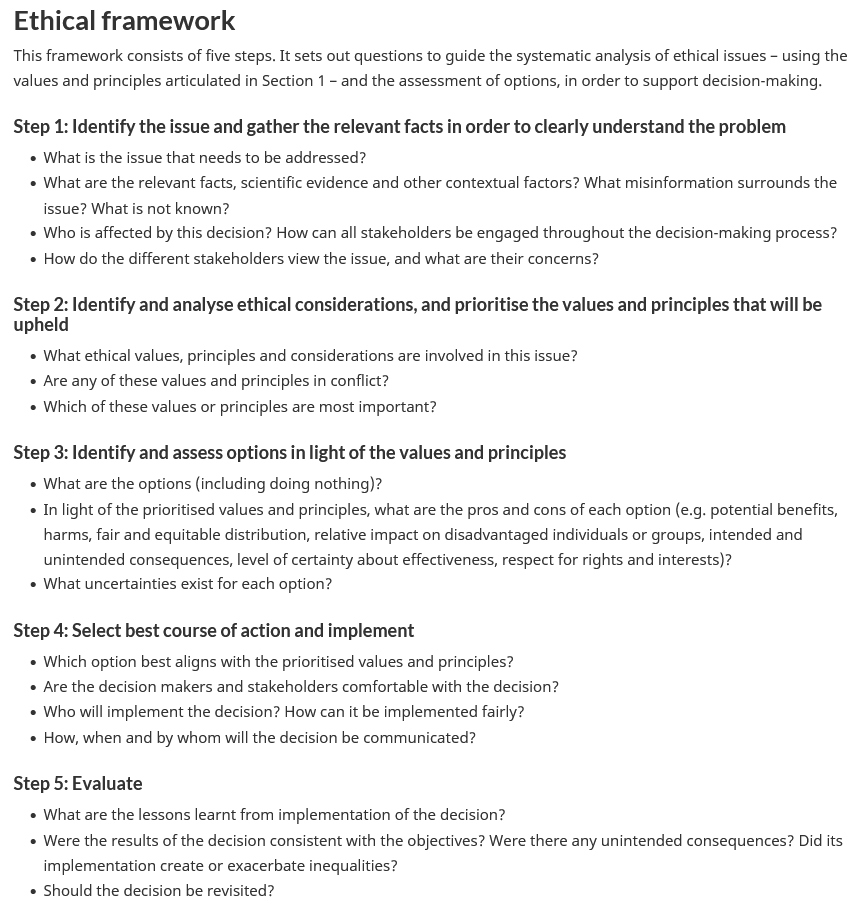
After this introduction and outline of guiding principles, PHAC’s ethical framework itself is a bit lame. It’s essentially a list of procedural questions organized by five steps that remind me of Simon’s (1960) framework for rational decision-making in management sciences, which consists of the intelligence, design, choice, and review phases. Canada’s “public health ethics framework” for the COVID-19 pandemic is shown in the screenshot above. I see some major gaps in Step 2 with respect to how to prioritize conflicting values and principles, and in Step 5 with respect to when to evaluate decisions, since monitoring should happen continuously in real-time with such critically important decisions.
Earlier, I highlighted one of the “ethical principles” of the guide: “Respect for persons and communities means recognizing the inherent human rights, dignity, and unconditional worth of all persons, regardless of their human condition (e.g., age, gender, race, ethnicity, disability, socioeconomic status, social worth, pre-existing health conditions, need for support).“ In a recent post, I criticized that human rights are commonly linked to a limited list of conditions, which is, in my view, a misunderstanding of the intended scope of human rights. Here in the PHAC framework, relevant aspects of dignity and (self-?)worth of a person are missing, e.g. their spiritual or philosophical view of body and soul; past experiences with Western medicine; and political opinions regarding the pharma industry or personal responsibility.
According to my notes from the meeting mentioned at the beginning of this post, my colleagues had expected that an ethical response to a public health emergency would, among other things, always pursue the least invasive measure and always balance community interests with individual autonomy. The “Respect…” section of the guide indeed cautions that “The right to autonomy is not absolute” but fails to provide much assistance in making related decisions. For example, I am missing a clear requirement that restrictions must be time-limited, regularly reviewed, and lifted immediately when found ineffective or obsolete; or an acknowledgement of red lines that cannot be crossed by the pandemic response, such as coerced or forced drug administration or other irreversible measures. I recommend re-reading entrepreneur and fellow Substacker Bill McMullin’s “Forced to take a risk to remain free” in this regard.
So far, the core theme of this post has only been mentioned in passing: the “public good” — what is this, who gets to define it, and how to weigh it against individual rights? In an interactive talk for The Ideas Institute, Prof. Bruce Pardy attempted to untangle the moral-legal questions around “What Are (Human) Rights?” Can it ever be ethical to sacrifice human beings to save the life of others? What protection does the constitutional right to bodily autonomy provide, if it is claimed by both sides of a debate, e.g. protection from an unwanted injection vs. (falsely assumed) protection from being infected by an unvaccinated person?
From a socio-political and personal vantage point, Toronto mayoral candidate Sarah Climenhaga had already explored “Freedom, Choice, and the Common Good” for the Toronto Moon in August 2022, as she was viciously attacked for showing an understanding for citizens who “would rather lose their job, lose their friends, be barred from family dinners or group gatherings, be called names, and have calls for their death spread on the front page of major media outlets” than take the mRNA injections.

In a book chapter included in The COVID-19 Pandemic (Ethics Press, see also here), higher-education standards expert Dr. Michael Tomlinson examines guidelines for “Balancing the Rights of the Individual with the ‘Common Good’”. He reviews existing pre-2020 pandemic response guidelines and contrasts their balanced, consensus-driven approach with the appalling new concept of “negative consensus”, i.e. proceeding with measures unless there is scientific consensus that they are not effective. Goodbye, precautionary principle!?
Tomlinson then reminds the reader of the principle of “non-maleficence” applied to government policies and argues that “public health agencies have an ethical obligation to undertake due diligence … to ensure that severe adverse effects of their measures are identified and considered.” Tomlinson himself provides numerous examples where this standard was not met, and most everyone reading this blog will know such examples too.
Around the same time in October 2022, Substack blogger Andreas Oehler explored the charge “You Have No Right to Endanger Others” made against unvaccinated individuals. In a way, this is the reverse of the position of those declining the mRNA “vaccines” on the basis of their questionable safety. Of critical importance, Oehler asks a question that I have grappled with: “What if the next jab is better?” Should everyone be expected to comply with public health mandates if they were demonstrably safe and effective?
In the context of discussing an article about the discrimination of the unvaccinated, I asked my colleagues on the Canadian Academics for Covid Ethics email list, to what degree they hold individual autonomy as an absolute value, or under what scientific or on-the-ground conditions they would concede the free-rider argument (made by vaccine believers against mandate opponents). The answers were unequivocal, such as the one received from Dr. Henryk Fukś:
Suppose that there is some common good in having a high percentage (or even all) vaccinated. Does this mean that people should be coerced to get vaccinated? My answer is: absolutely not. The view that the use of force and coercion by the state is justified as long as it serves the common good is based on a very distorted view of common good. The common good, as St. Thomas Aquinas argued, is based on free and reasoned acceptance of truth.
Or another colleague arguing from a historic perspective:
When I first started reading “common good” arguments early in Covid, I couldn’t help but recall reading at some point the 1920 Nazi party slogan, “Gemeinnutz geht vor Eigennutz”. Participating in the common good requires the lack of any coercion, or it ceases being a good.
Or Dr. Laurent Leduc’s response, speaking from the Socratic viewpoint:
Back in 1869 there was one science journal which had perhaps 40 pages. At that time scientists could read about all the frontiers of knowledge, discuss those and debate. Today we have mass confusion around what we think we know and we go ahead acting in accordance with that ‘thinking that we know’. For me, bodily autonomy trumps the ignorance of which we are ignorant.
Or Dr. Claudia Chaufan from a more practical angle:
No medical intervention should be forced on any grounds, “common good“ or other. Besides, I don’t know of one case in history in which claims from “the science“ about an alleged common good stood the test of time, and too many that proved to be simply organised fraud and crime. And even if examples did exist in a “what if“ scenario ... I think personal autonomy is too fundamental a value. At any rate if I ever had any doubts, policies to achieve the “common good“ during these last few years have swept them away...
While advocates of mandatory vaccination argue that individuals have a responsibility to be vaccinated for the benefit of public health and to protect those who cannot be vaccinated, Michael Kowalik demonstrates that this conclusion is flawed. In “Ethics of vaccine refusal”, the author contends that there is no moral or ethical obligation to vaccinate, even if a vaccine was 100% safe, and that “[bodily] autonomy … has absolute normative priority over reduction or elimination of the … risks to life.”
Kowalik therefore concludes that vaccination mandates are discriminatory towards healthy individuals based on their biological traits and contradicts established ethical principles. In other words, the author argues that our natural body state cannot be made illegal. After reading this article, the concept of “inalienable rights” makes a whole lot more sense to me. As does the refugee advocacy slogan “no one is illegal”.

In Plato’s cave allegory, a group of prisoners grew up only seeing shadows of real-world objects, not the objects themselves. They lived in a much-reduced reality of black-and-white silhouettes within a cave. If a prisoner was allowed to move about and discover the three-dimensional objects casting the shadows, he might be blinded by the fire that created the shadows and much prefer turning back to the familiar sight of the silhouettes. If a prisoner was taken out of the cave to see an even richer reality, he would be blinded even more. However, if the prisoner got used to the light, he would understand that the objects in the cave and, even more so, their shadows represent a much reduced reality. Yet, if this person was to return into the cave, he would be unable to see in the darkness and have a very hard time convincing his fellow prisoners of the value of the higher level truths.
The “common good” seems to me to be such an “object”, perhaps among very many COVID-era “objects”, which the many “prisoners” of societal conventions, conveniences, and comforts are perceiving in a much-reduced shape. I hope this post and the outstanding work by many critical social scientists and humanities scholars is starting to shed more light into the dark corners of the mainstream narratives.